Do you hear your child snoring at night with pauses, snorts or gasps?
Heavy Breathing while sleeping?
Very restless sleep and sleeping in unusual positions?
Does your child have shortness of breath?
Daytime sleepiness or behavioral problems?
Bed wetting (especially if your child previously stayed dry at night)?
If any of the above symptoms describe your child please read on, as a new study in the journal Sleep and Breathing found that rapid maxillary expansion (RME) was effective in treating obstructive sleep apnea (OSA) in children. The results of the treatment were clearly visible two years after the treatment has ended. RME involves widening the jaws using oral appliances by enlarging the maxillary dental arch and the palate (roof of the mouth) to re-establish balance between the width of the jaws.
The researchers evaluated the target and instinctive data over a 36-month follow-up period to determine whether RME has been effective in the long-term treatment of OSA. The study included 14 children. The children’s main age was 6.6 years at start of treatment and 9.7 years at the end of follow-up treatment. Each child underwent an orthodontic assessment to detect possible jaw irregularity from normal occlusion: deep bite, retrusive bite and crossbite.
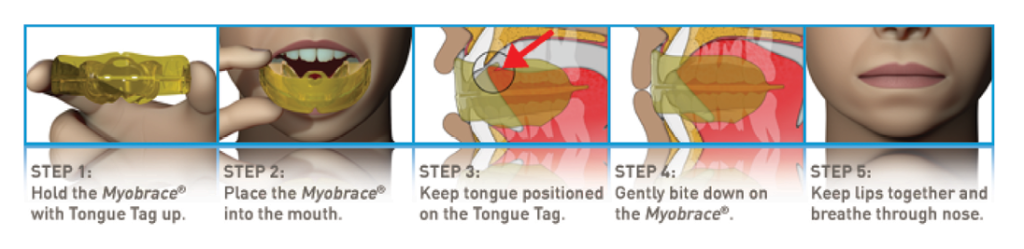
A high angle face can cause breathing problems for children. Another common cause of OSA is large tonsils or adenoids. Removing the tonsils or readjusting the jaw line can help children breathe more easily during sleep, but before going into the surgical rout there is another option called MYOBRACE. MYOBRACE (see figure at the bottom of the page) is an appliance which is designed to be used in-sequence to effectively train the tongue to position correctly in the upper jaw (known as the tongue spot), retrain the oral musculature and exert light forces to alight the teeth. This appliance can be used on children as early as 3 years old.
All 14 children completed a 12-month therapeutic trial using RME, where 10 enrolled in the follow-up study. Of those 10 children, 5 were male and 5 were female. The 10 children took an overnight polysomnography (PSG) to test for the presence of OSA at baseline, after only one year of follow-up treatment, and two years after treatment completion. Results showed that the apnea-hypopnea index (AHI) diminished and the original clinical symptoms had resolved by the end of the treatment period. Twenty-four months after the treatment has ended, no notable adjustments in the AHI or in other variables were noticed.
To learn more about early childhood treatment of sleep apnea or MYOBRACE please visit our website www.sunrise-orthodontics.com and The American Academy of Dental Sleep Medicine—www.aadsm.org, where the original article was published.
Myobrace can also be used on children with or without braces.